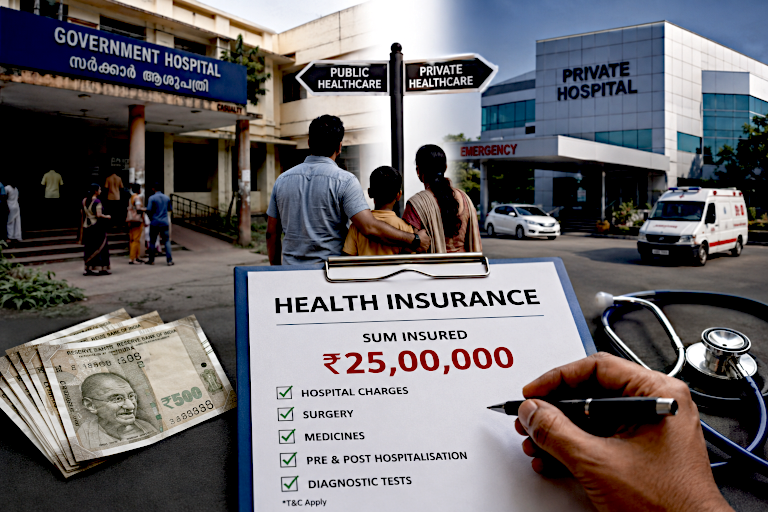
Kerala has long taken pride in the strength of its public healthcare system. However, incidents during the previous government’s tenure revealed a system under severe strain and often poorly managed. Chronic shortages of funds have plagued public healthcare for years.
The new UDF government’s proposed alternative — if it can indeed be called one — is an insurance scheme offering coverage of up to ₹25 lakh for every family, though it remains unclear who exactly will be eligible. In effect, the government will be encouraging patients to shift from public hospitals to private ones. Such a move is likely to do more harm than good.
Private healthcare services are already expensive and, in many cases, exorbitantly priced. As demand increases, costs are bound to rise further. Insurance coverage can also reduce price competition, contributing to spiraling healthcare expenses.
It seems that the multi-national companies had sensed or managed to bring about the shift in health care sector from public to private sector. They have brought hospitals even in medium towns. Several private hospitals are already notorious offering unnecessary procedures and over-charging patients. Now, the government will be aiding them to expand business.
The government hospitals in the State have best of doctors, nurses and paramedics. On the other hand, doctors who studied in dubious medical colleges in India and abroad find placement in some private hospitals. Poor and less-informed patients are especially vulnerable to being misled in such institutions. While government hospitals may suffer from neglect and shortages of resources, patients there are generally less likely to be subjected to unnecessary procedures and medication. Addressing shortages of funds, infrastructure and staff should therefore be the primary responsibility of the new Kerala Health Minister, K. Muraleedharan. If universal health coverage is indeed the goal, it would make more sense to invest the insurance premium funds directly into strengthening government hospitals.
Insurance-based healthcare may also burden poor and less-educated patients with bureaucratic hurdles. Insurance companies could deny claims, demand prior approvals or insist on complex documentation before treatment is provided. In some cases, patients may even need legal assistance. Anyone familiar with motor vehicle insurance knows that workshops often charge differently for insured and uninsured vehicles. The same pattern is likely to emerge in healthcare billing, ultimately driving up insurance premiums. If the government proceeds with its “Indira guarantee” for health insurance, it may soon find itself facing ever-increasing costs.
Ayurveda and Homeopathy
Kerala’s healthcare landscape is also distinguished by its large number of institutions offering treatment under Ayurveda, Homeopathy and Siddha systems. Medicines used in these traditions produce fewer side effects. At the same time, there is a growing view that some of these systems — particularly Homeopathy — lack a scientific basis.

Ayurveda continues to attribute disease to imbalances in Vata, Pitta and Kapha — concepts associated with movement, metabolism and structural stability — and does not fully incorporate the modern scientific understanding that germs cause disease. The government should therefore take steps to modernise Ayurveda by integrating contemporary medical knowledge into its curriculum. Even if traditional concepts such as Vata, Pitta and Kapha are retained, modern scientific understanding should be logically connected to them.
Ayurveda, Siddha and Unani cannot easily be dismissed as pseudosciences, since they evolved through centuries of observation, experimentation and inference — methods that broadly align with scientific inquiry. The same cannot be said of Homeopathy. There is no convincing scientific evidence that highly diluted homeopathic remedies are effective beyond the placebo effect. Moreover, many homeopathic medicines have not undergone rigorous testing. Many practitioners are known to mix modern medicines with homeopathic medicines to show results.
The government should therefore commission independent studies to evaluate the efficacy of homeopathic medicines using modern research methods. Until such studies are completed, public expenditure on homeopathic institutions should be curtailed. No new homeopathic dispensaries, hospitals or medical colleges should be established. Medicines used across AYUSH systems should undergo rigorous scrutiny, and any harmful substances should be purged from the official Materia Medica.
Any attempt to modernise AYUSH systems and their curricula is likely to face opposition from sections of the modern medical establishment. However, it is worth remembering that allopathy itself evolved over time into what is now considered modern medicine.